One of the challenges of being a rural doctor is the need to stay abreast of knowledge and skills across a wide variety of fields. More than “just a GP”, our work encompasses primary care for sure – but also on call responsibilities for emergency, anaesthesia and obstetrics. My colleague Casey Parker over at BroomeDocs likens the rural doc to a ‘swiss army knife’ – not as precise as the surgeon’s scalpel…but a heck of a lot more useful when dealing with a multitude of problems.
One of the hardest challenges for rural hospitals is dealing with infrequent but challenging emergencies – certainly the maxim ‘critical illness doesn’t respect geography‘ holds true in rural Australia. I’m interested in ways to help rural docs deliver quality care, out there – FOAMed helps us to keep our knowledge up-to-date to a degree (Casey and I published on this last week, in a journal article that ironically took >12 months to get published, when same content was out on our blogs ages ago!)
For critical illness, I maintain that rural hospitals have a LOT to learn from the prehospital arena. Simulation training, standardisation, use of SOPs and action cards are all common practice for prehospital services – but not yet embraced by responsible bodies (Country Health SA in my neck of the woods).
The difficulty in rural…
Last year I spent some time withe MedSTAR, the SA retrieval service, partly to see how they do it, but also to gather more information on the way in which critical illness is handled at other locations in my State of South Australia.
It was an interesting time. Whilst MedSTAR didn’t quite meet my expectations in terms of training, audit and effectiveness, I was also saddened by the heterogeneity in care between rural hospitals – some were excellent, the majority quite hum-drum and a few frankly dangerous.
In part this is to be expected – a small rural hospital may only encounter a particular critical condition infrequently, leading to de-skilling of staff. Similarly access to equipment may be lacking, as may be familiarity with use (the inability to deliver NIPPV or run inotropes seem to be common failings).
To ensure a robust response to the critical patient requires organisational change – leadership from within CHSA, on-the-ground champions to ensure clinical staff education, embracing the concept of both task-training and in situ team-based scenario sim…and also audit of retrieved cases. Incremental changes – to make things better. Sadly there appears little scope within CHSA to drive such change from the nominated chief consultants – or perhaps a lack of willingness to listen to them? At an individual hospital level, nursing staff are hampered by having to repeat annual mandatory training from fire safety, manual handling, hand-washing, drug-labelling, ALS etc. As a result, a certain minimum level is measured – but there is scant spare time to meet more challenging educational needs, such as sepsis, human factors, critical airway, paeds emergencies etc. Every year, doctors and nurses prove their competency in BLS and ALS – but are rarely required to prove competency in dealing with a critical patient unless he/she has arrested!
“annual mandatory training ensures a standard level of competency – I am relieved to now that none of the nursing staff will injure their backs in a hand-washing fire – but allows little scope for developing educational needs and institutional readiness for critical illness”
So if CHSA lack the leadership to raise the bar and individual nursing staff are snowed under with mandatory training, what scope is there to improve? At an individual level, doctors and nurses can tap into the rich resources of disseminated web 2.0 knowledge via FOAMed. A few do – but my experience is that some rural doctors adopt a ‘wait for retrieval to sort it out’ approach…which sticks in my craw somewhat.
Shared SOPs and Action Cards
The experts in critical care in rural areas are, undoubtedly, the retrieval service. Sure, there are some blindspots (some of the retrieval coordinators may have no idea of what it ‘out there’ and may, justifiably be concerned at the lack of skill in rural, adopting a ‘hands off the patient until we arrive’ approach). I see great scope to share the tacit knowledge of retrieval expertise with rural clinicians – after all, we are dealing with the same patients!
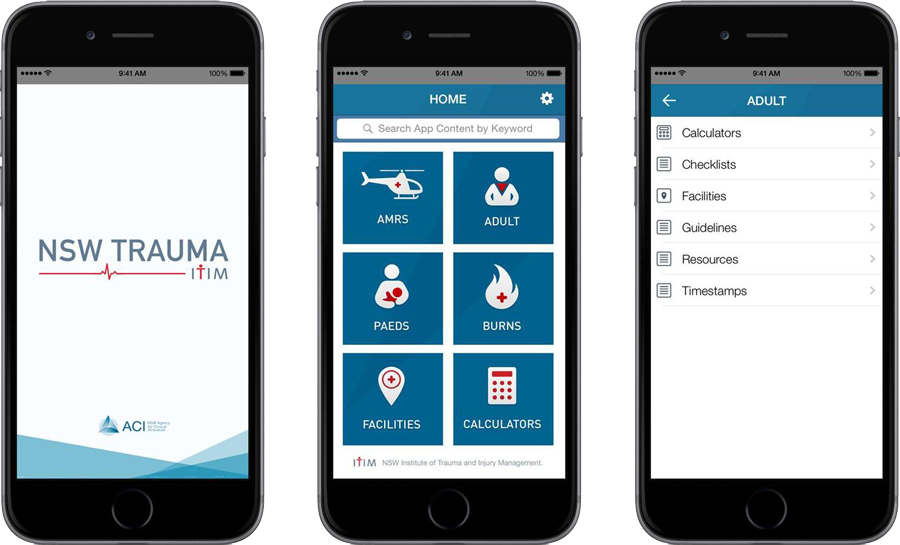
So this week I was pleased to see both Emergency Medical Retrieval Scotland (EMRS) and the NSW Institute of Trauma Management release some SOPs and Action Cards via website & app respectively. If you haven’t already – check them out!
Download the NSW Trauma App here : http://www.aci.health.nsw.gov.au/networks/itim/about_itim/trauma-app
Now I’ve blogged on the value of such resources being made available before – EMRS and UK HEMS have made their protocols available online for over a year; Auckland HEMS made their checklist app available to all to share. But the value, for me as a rural clinician, is having resources that are locally-relevant – I would love to see a similar slew of resources made available to rural doctors in SA, particularly as standards seem to vary widely and there is no serious local leadership within CHSA…nor audit of retrieval cases by CHSA.
The ITM app is slick – easy to navigate buttons, packed full of checklists, action cards, SOPs, CPGs, calculators, contact details – and relevant for both large centres and smaller rural hospitals. In short, all the info you need, in your smartphone, tablet or PC, whether a rural clinician, a retrievalist or a receiving facility. Kudos. There should be the same in every State!

I cannot emphasise enough how valuable such resources are to the rural clinician – having access to shared protocols seems a no-brainer….as does the possibility of driving improvement in care of the critically ill in rural by such tacit knowledge sharing.
The future?
It would be great to have an app or access to retrieval protocols allowed to be disseminated to rural clinicians in SA. Ideally content is specific to local needs and building capacity and hopefully driving future improvement in care of the critically unwell. Is it the responsibility of the retrieval service to deliver this content? I am not sure….in these times of financial austerity there may be little spare capacity or cold hard cash to deliver. Nor may there be a will. Personally I think that the desire for improvement HAS to come form the rural clinicians, although as private contractors we have little influence over standards and training in CHSA hospitals.
There’s an old phrase “the standard you walk past is the standard you accept“
I think we do have a problem with varying standards of care in rural Australia. Admittedly there is a huge problem with recruitment, which may lead to inexperienced or deskilled clinicians being placed in isolated rural areas with primary care skills alone, then expected to deal with emergencies. Having to bail these places out will put a strain on retrieval services which may come to expect the lowest level of care as standard from rural facilities. This saddens me, as I don’t agree with the adage of “better a bad doctor, than no doctor” and am keen for both rural doctors to raise the bar, CHSA to get serious about quality improvement and of course guidance from retrieval.
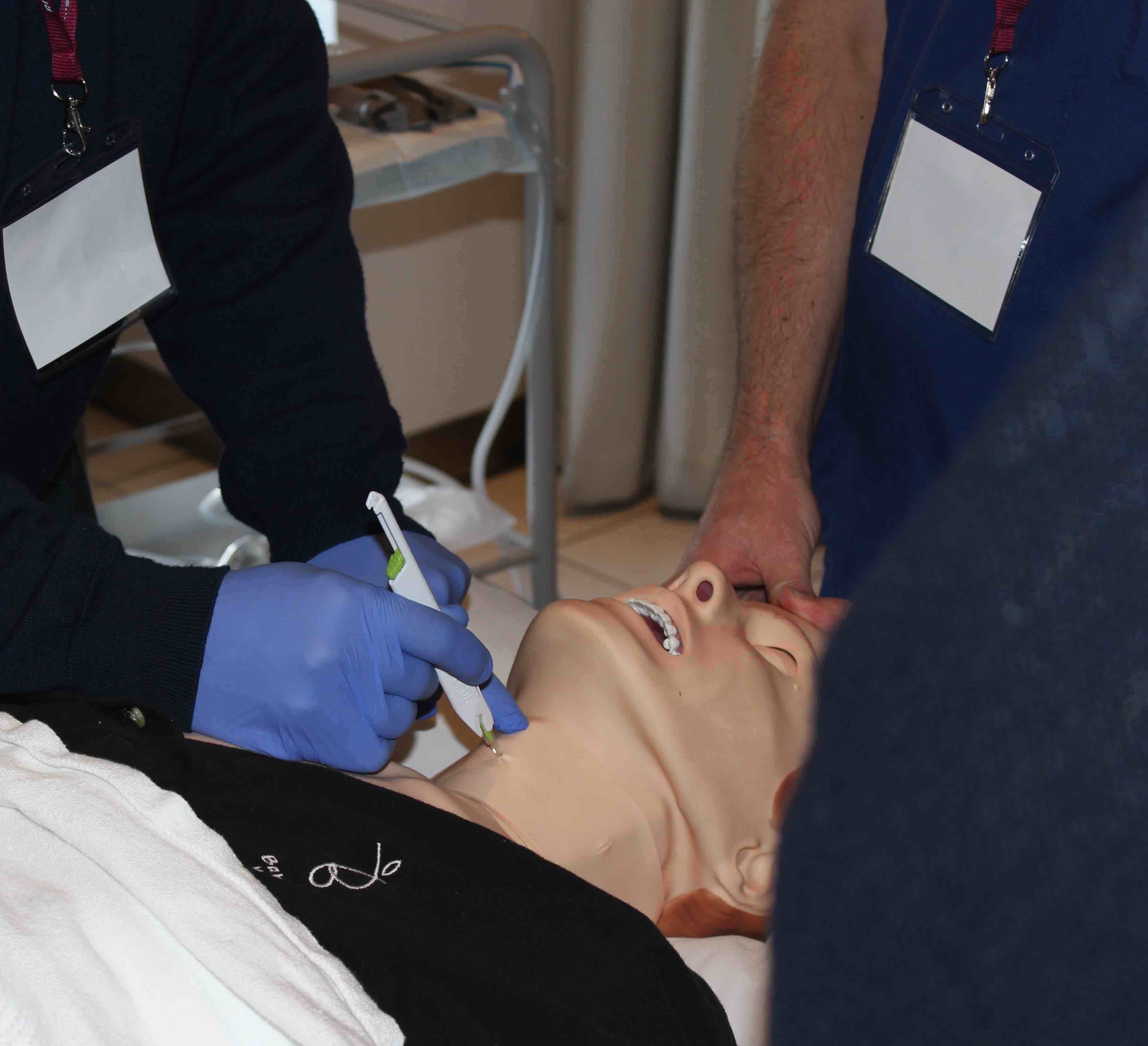
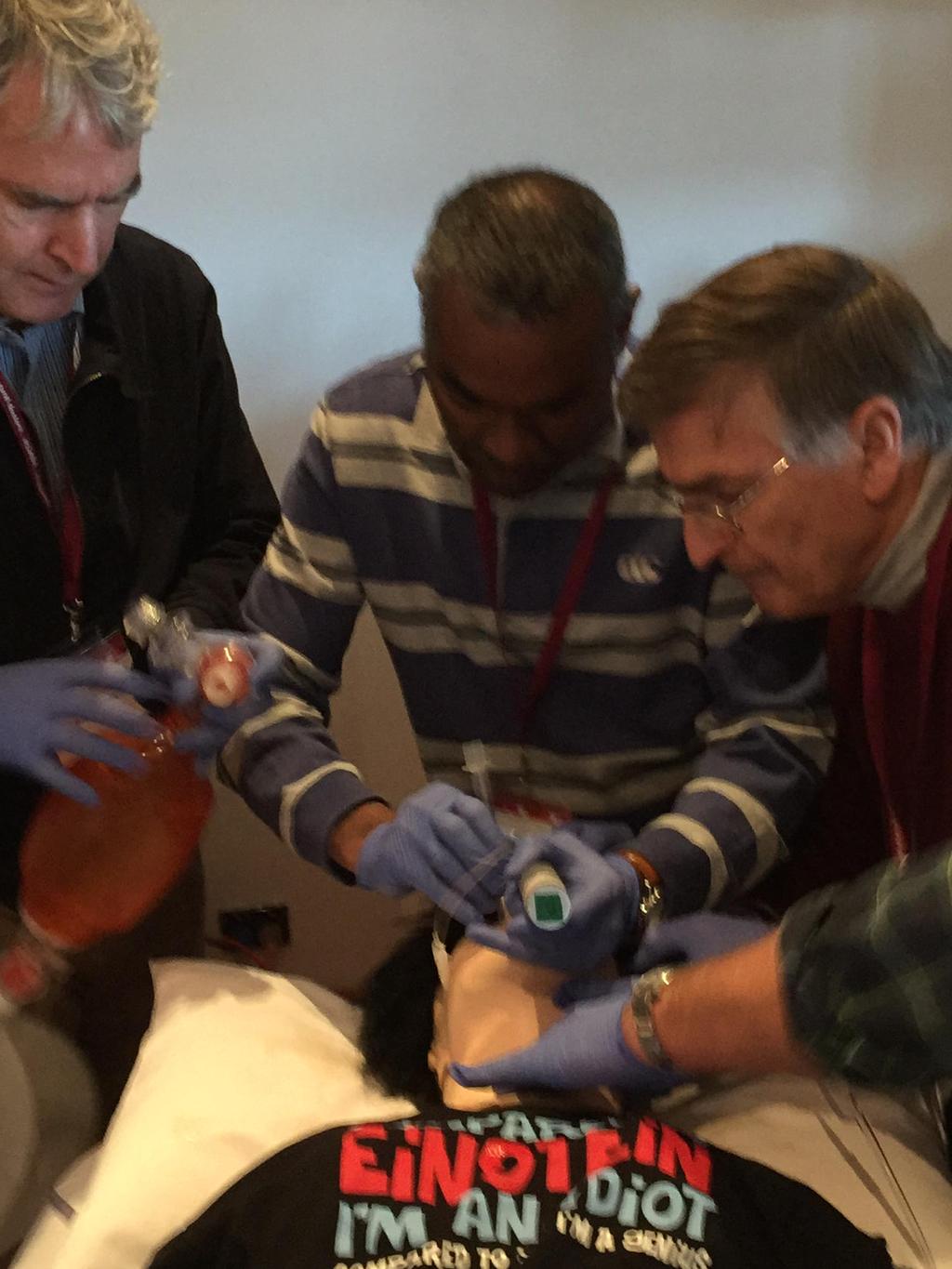

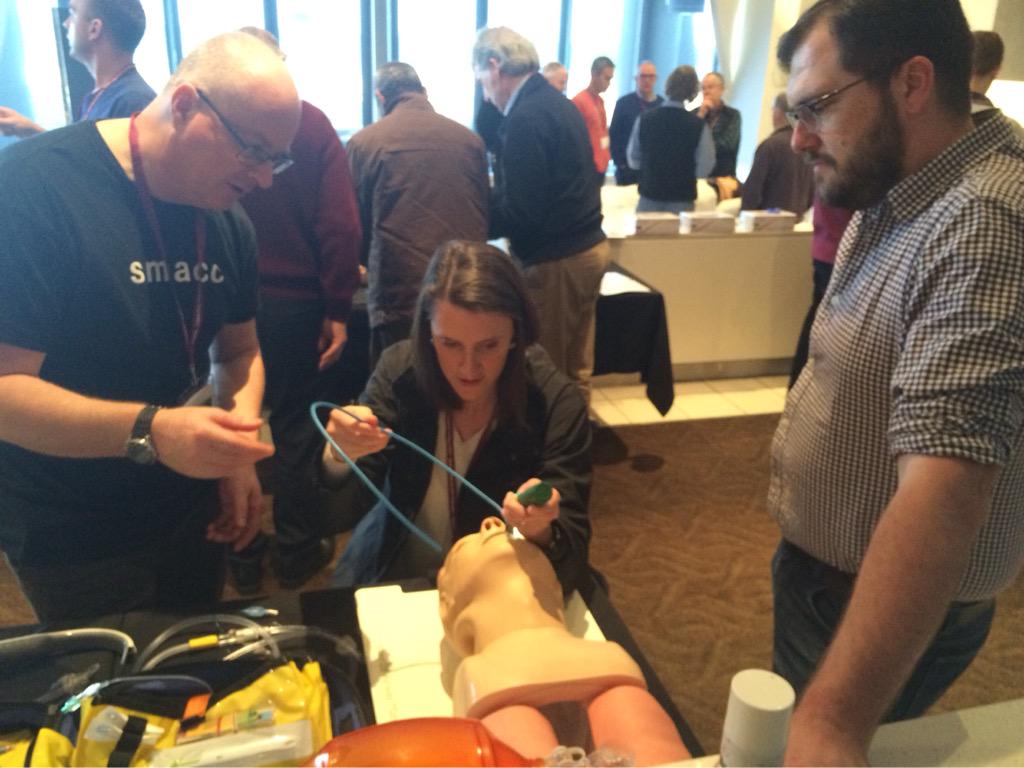

Above – Rural Docs Masterclass (Airway session) inc. elements of the smaccAIRWAY SALAD Sim (vomit)
Three steps towards better trauma care in rural SA?
- encourage rural clinicians to embrace care of the critically ill – this is scary for the occasionalist, but requires not just repetition of the lowest common denominaotr alphabet courses such as RESP, but to attend annual RDASA Masterclass and encourage use of FOAMed
- CHSA to take ownership of their rural hospitals – embrace standardisation of equipment and training, use of action cards, encourage nursing staff to deviate from usual mandatory training and upskill in relevant areas, conduct team-based in situ sim training and to audit retrieval cases (and involve local doctors in this process!). Good clinical governance, not meeting tick-box standards
- retrieval and tertiary centres to facilitate knowledge sharing – web 2.0 tech such as the ITM app and EMRS site with SOPS, CPGs, checklists, calculators and so on are invaluable
Of course, at a meta-level social media and FOAMed allows inter-agency benchmarking, to a degree. I’m a fan of the HURT Registry, designed to help prehospital services compare their approach to major haemorrhage. Have a look at the map – plenty of scope for other services to join up…
All of this would go a long way towards improving standards. But we have to want to change…