Truth of the matter is that most of the emergencies in my tiny rural hospital ED are relatively straightforward – injured bones, psychiatric emergencies, infections, cardiac conditions and so on. Every now and then we are challenged with a patient requiring retrieval, but most of those need either meticulous monitoring, inotropic support or transfer to definitive care. Airway management is a very small – but important – part of the remit.
So therein lies a problem – despite the nature of ‘occasionalism’, how can the rural team keep on top of their game? It’s all very well having knowledge – but practical applicaiton may disintegrate under cognitive load or a crisis. To my mind, simple things can help mitigate against ‘occasionalism’, such as
– standardised equipment
– in situ multidisciplinary sim training
– and use of appropriate cognitive aids
For my money, the Vortex is simply the best cognitive aid to use in managing an unanticipated difficult airway, allowing team members to communicate and decide on best optimisation strategies before moving to next ‘lifeline’
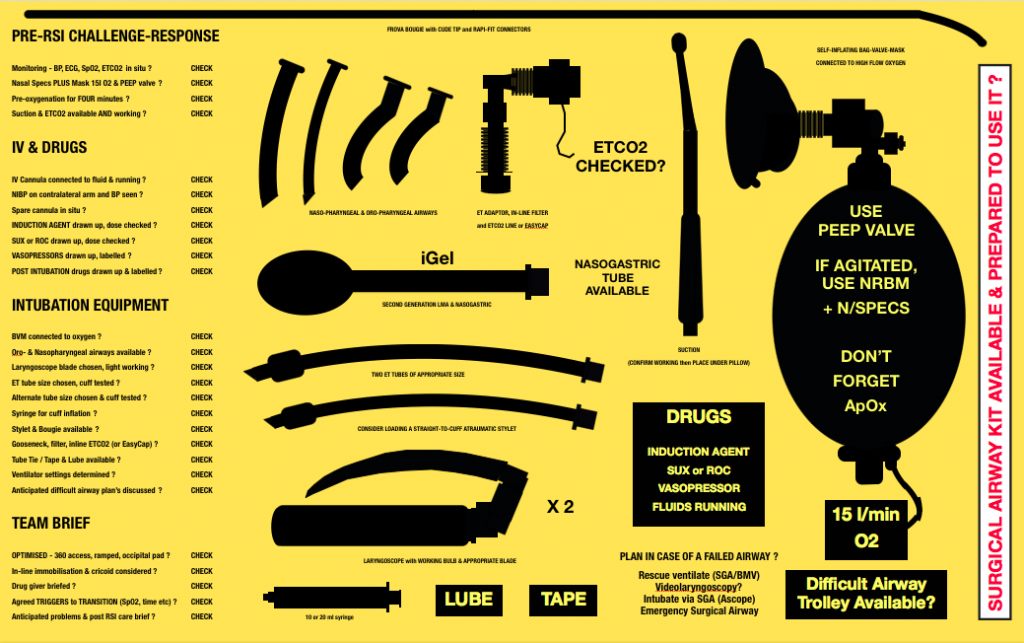
But if we get pre-notification of a sick patient coming in, or if we decide to ‘set up’ for an ED RSI, then having a ‘kit dump’ can help even the unfamiliar team assemble the correct equipment AND to decide on an appropriate airway plan.
I’ve been using this one, adapted from London HEMS (then adapted from Sydney HEMS, MedSTAR SA) then shared on amongst RFDS Qld and WA rural EDs.
But it’s a bit dated and has been superseded in many locations by a dedicated RSI ‘checklist’ and tools such as the SCRAM bag (structured critical airway management bag)…
The SCRAM bag….my fav piece of airway kit….
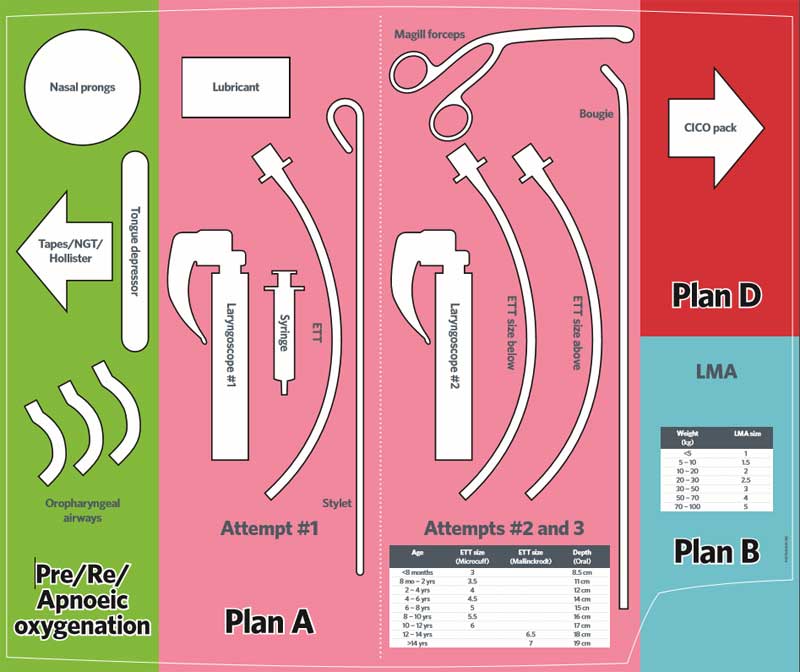
 So I was intrigued when I saw THIS kit dump, which I believe is attributed to the Melbourne Children’s Hospital ED.
So I was intrigued when I saw THIS kit dump, which I believe is attributed to the Melbourne Children’s Hospital ED.
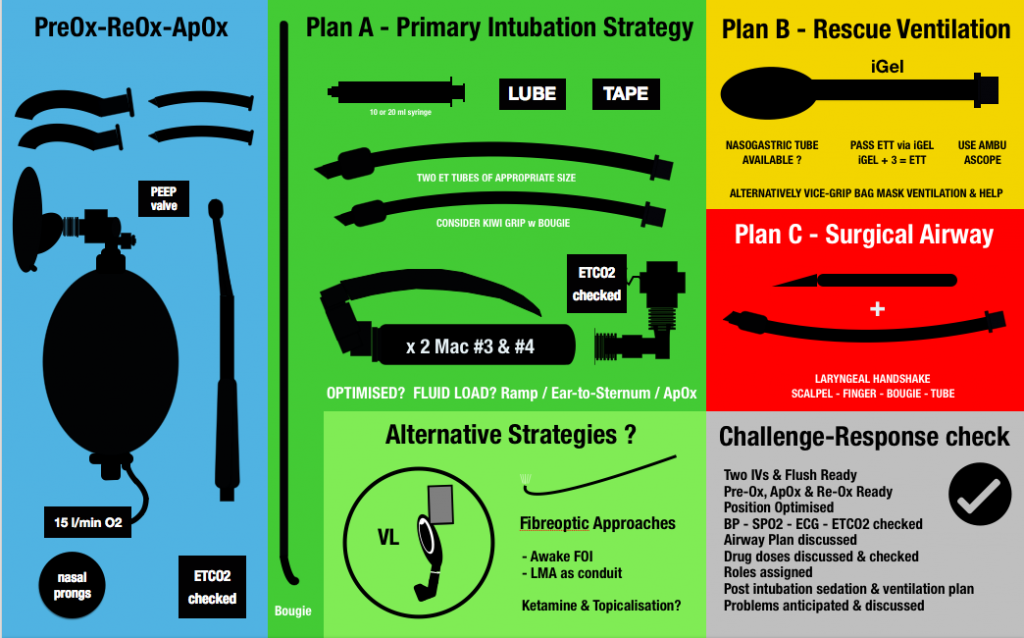
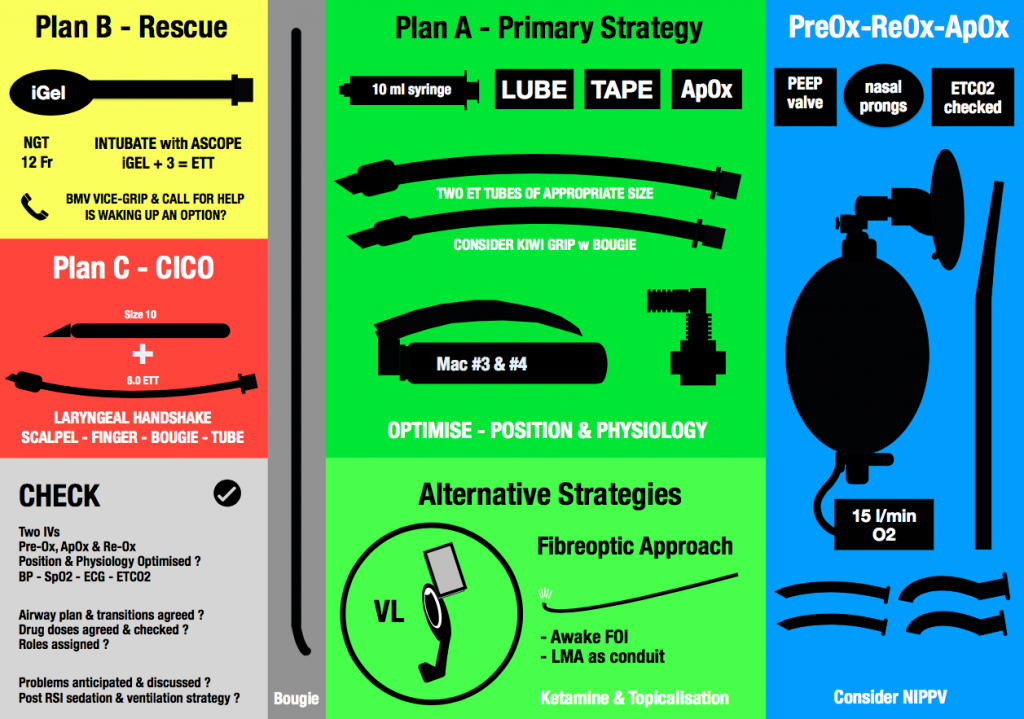
Based on that, I’ve re-jigged my RSI kit dump. The original file is designed to be printed out in a large size, about the size of the top of the Resus trolley. The aim is to both assemble appropriate equipment reliably without omission…and to encourage the team to consider their airway plan.
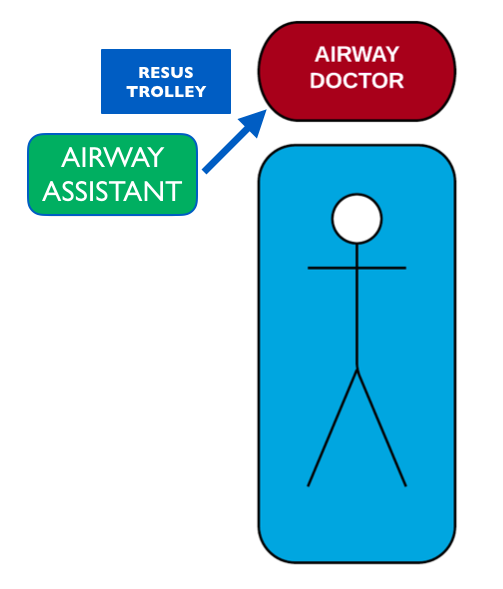
Then I started thinking about the layout in a little more detail. For our set up, the airway trolley usually sits to the right side of the patient. The airway assistant faces the trolley (so he/she can access the drawers) and so passes equipment to the airway clinician responsible for intubation.
Problem is, the logical left-to-right sequence of PreOx-Plan A-Plan B-Plan C means that commonly used equipment is furthest away from the airway operator….and can knock over rescue SGA and CICO kit.
So I’ve deliberately reversed the set up, such that the PREOX (blue) is closest to the operator…followed by Plan A (primary intubation strategy). Plans B and C are nicely tucked off to the side. I’ve also swapped out the Yankauer sucker for a DuCanto!
Does this work? Well it does for me…but you might want to adjust and make your own….
My dream? One of these in every rural ED…along with the kit to make it work…supported by in situ multiD sim updates and regular case audit….
Enjoy!
Hi Tim! Cynthia from the Northern Melbourne here. Thanks for this. We were in the process of making a similar shadow diagram for our ED, with the hopes of standardising airway for the hospital. Any chance we can use your diagram/template please?
Same as Cynthia here Tom. SA Para looking at this as a shadow board/kit dump. Are we able to use your diagram/template please?
Hi Tim, I would love to implement this at our facility. How can I download or obtain your kit dump?
Hi Tim,
Where did you get the black outlined pieces of kit images from?
Cheers, Tom
Hello Tim, loved reading this.
I am in the middle of creating a kit dump for our rural hospital. Really needing some images though as Im not too creative to make my own. Can chance you’re able to send these through?
Kind regards