My blog profile mention that I am an instructor and course director for the ATLS-EMST course. ATLS-EMST is something in which I believe – a structured approach to trauma management training for doctors. But over the years I have become frustrated with the tardiness of knowledge translation – concepts that I learn about via FOAMed will take many years to trickle down onto courses such as these. There needs to be something better. For the rural doctors, we conducted a FOAMed-based ‘rural masterclass’ on Kangaroo Island which was well-received. On the same weekend, Drs Amit Maini and Andy Buck held the inaugural Emergency Trauma Management course in Melbourne. I managed to get along to the second course along with 23 other doctors including Dr Jeram Hyde. He has kindly consented to write a review of ETM. Now read on…

EMERGENCY TRAUMA MANAGEMENT COURSE – REVIEW
Dr Jeram Hyde is a Critical Care Registrar in ICU, ED & retrieval medicine, who loves working in regional trauma centres. He collects watches & naps whenever he can. Views are his own, & in no way reflect the views of his employers or professional Colleges.
“High on content, low on lectures, pragmatic approach rather than dogmatic, huge emphasis on modern best practice & #FOAMed concepts. Amazing facilities & stunning food”
On the weekend I had the pleasure of doing the new Emergency Trauma Management Course (aka the ETM Course) in Melbourne, and finally managed to catch up with Tim after a bit of a twitter bromance over the past while. We’ve both been extremely excited about the course and I’m happy to say it didn’t disappoint! If you haven’t already checked out the courses website, check some of their content e.g. Thoractomy Critique and their course manual.
What is ETM?
ETM is a brand new trauma management course, the brainchild (lovechild even?) of 2 of the nicest guys out there: Andy Buck and Amit Maini. Andy and Amit are both FACEMs and trauma nuts from Melbourne and have only just started running ETM in late 2013 after over a year of planning.

Why ETM?
The question everyone has been is asking is why ETM? Surely trauma has been covered more than enough through ATLS/EMST running all over the world? Well I’d beg to disagree, and thankfully the guys at ETM do too.
ATLS has done an amazing job in bringing standardised trauma care around the world, and gives an excellent grounding in trauma management for junior doctors in surgery, ED, ICU, anaesthetics etc who will be managing trauma. But it’s own simplicity and generalizability is ATLS’s greatest strength and weakness. ATLS provides a solid grounding, but it does leave a gap in the ongoing education of doctors in managing trauma, namely – how do you function and manage trauma when you are no longer in the idyllic single doctor rural ATLS scenario. What about when you’re instead a senior ED Reg or consultant in a busy trauma centre, having to manage a trauma team you’ve never met before ? How does the linear ABCDE alphabet approach work then, when there are competing priorities, personalities and top level decisions to be made between theatre, imaging, angioembolisation or retrieval elsewhere?
Andy and Amit have tried to develop the course to help fill the perceived gap out there in advanced, up to date, trauma management and team leading skills. The course was born out of an experience the two of them had a few years ago whilst working in a trauma centre where they witnessed a senior, and otherwise extremely competent, ED registrar bungle a straightforward trauma. On debriefing afterwards it became clear that despite having done ATLS/EMST and having a theoretical framework for trauma management, the registrar was having difficulty translating that into real world practice with difficult personalities within the trauma team and competing urgent management decisions. This is obviously a common experience held by many around the country, judging by my own experience and Cliff Reid’s excellent talk at SMACC this year on Making Things Happen in resus.
Where is the course?
ETM has a perfect location: right in the CBD of Melbourne. 1 block from Flagstaff train station. Those who’ve been to ACEM headquarters before will be familiar with the area, as ETM’s headquarters is only 2 blocks away.
For those cofee addicts out there – don’t worry, being Melbourne there is coffee provided at the course, and some great coffee available on the walk from the train station to the course. Tim was more delighted about the nearby Japanese restaurants and numerous bars.
The guys have obviously put a huge amount of effort into the course, and it shows. The course is run in a dedicated office space that the course has rented and developed, with a lecture room and multiple sim rooms.
So how was the course?
In short, well worth it. It was an absolute thrill to attend a trauma course designed for modern day practice and written and run by people who actually are doing trauma management daily. I particularly found it exciting to see so much up to date medical practice pervading the course. Just on the first day alone the course covered so much recent #FOAMed content and modern practice such as apnoeic oxygenation in the trauma intubation, 1:1:1 blood product resuscitation, airway checklists, The Vortex, CABC approach to massive haemorrhage in trauma, use of PEEP valves in pre-oxygenation etc etc.
One of the key themes that came through the course over the 3 days was a the key of having a “pragmatic not dogmatic” approach to trauma management. The course is also quite high on content and ‘doing’ in sim scenarios, rather than the death by powerpoint approach some other courses take.
Day One covered the basics of resus room setup, and trauma reception. There were skill workstations on the trauma basics of finger thoracostomies, insertion of rapid infusor cannulas (RIC lines – a personal favourite of mine), IO insertion, pelvic splinting, bougie intubation etc . The simulation scenarios on day 1 were quite basic with only single “life threats” (e.g. trauma pt with only a tension ptx). These initial sims and lectures were extremely well run and the workshops were valuable to anyone who hadn’t put in IO’s or RICs before, but to be honest by the end of day one I was a bit worried the course being being pitched a bit too low for what I was expecting. The sim scenarios on day 1 were pitched at the level of final day test sims on a ATLS course, and were run with just 1 doctor and 1 assistant.
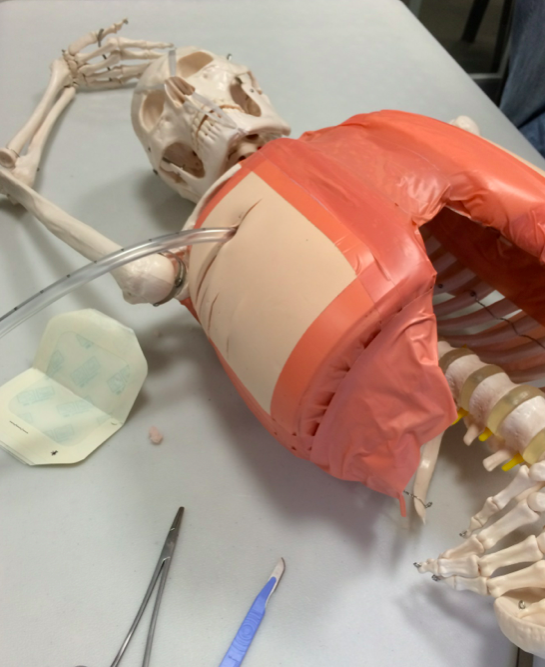
(ignore the anterior placement – we ran out of rib spaces)
Needless to say these fears were allayed promptly by the course taking everyone out to the pub for drinks (on them!) at the end of day one.

(Clockwise from bottom left – me, Andy, Tim)
My concerns disappeared faster than roadkill on Kangaroo Island at the beginning of day two. The sim scenarios jumped up a gear, and the ‘single doctor + assistant’ team morphed into a 4 doctor advanced trauma team. The ‘patients’ became sicker and had 2 or more life threats. No longer could the trauma team afford to do things sequentially – simultaneous RIC access, decompressive thoracostomy and setting up for a difficult intubation for a traumatic brain injury in a hypotensive patient were required, with the team leader now finally able to stand back and not be physically involved, but rather lead as we do in real life. Xrays and FAST images were displayed when requested, and not every cannulation or intubation attempt was successful in the scenarios. It was great to see difficult airway management (rightly!) become a trauma management issue as well, as the team leader has to weigh up risk/benefits of the TBI with low GCS and multiple facial fractures being intubated now by ED RSI, or in 20 minutes by anaesthetics.
But even more exciting than the realistic sim scenarios was the huge emphasis placed on Resus Room Management (RRM) and the huge gap between the usually taught ‘Crew Resource Management’ (CRM) techniques used in stable teams such as the airline industry, and the dynamic teams (or flash mobs of strangers) that often make up the rotating roster of trauma teams. Sessions were spent practicing closed loop communication, and a lot of educational effort was put into helping us develop better leadership and communication skills that translate back into our own busy and chaotic resus rooms.

Final day workshops included surgical airways, ED resuscitative thoracotomy (always a crowd pleaser!), difficult airway management and retrieval considerations for trauma patients. The thoractomy workshop was great fun as expected, with the chance to crack open their resident skeleton Bob’s chest. Understandly animals weren’t used – as you’d need a single sheep per participant for everyone to be able to do their own thoracotomies.

Overall I ended up loving the course, despite my initial reservations after the first day. Whilst it started out at a EMST/ATLS level course on day one, that was simply the building blocks for diving into more complex and realistic trauma cases over the next 2 days. By the end of day three, the scenarios would have 3 concurrent life threats that all required immediate action, as well as ongoing assessment and management decisions. I particularly valued the change up that happened on day three, when they took us out of the group of 5 doctors you’ve been with for the past 2 days, mixed up the groups and threw us into even harder sim scenarios with strangers you haven’t worked with before. Great way to practice clear, closed loop, communication.
Which brings me to a few final points:
The lack of animals… initially I thought the course would suffer for this, but after the weekend I didn’t miss them at all. ETM Course has invested heavily in some great models and the time saved from not having to travel to an animal lab was well spent on other workshops.
The food –was amazing! Provided by the Asylum Seeker Resource Centre, we had stunning vegetarian & halal food (and sometimes vegan) meals provided 3 times daily. As a devoted carnivore myself, I thought this would grow tiresome as vegetarian food I usually find repetitive… but the variety and flavours of the food were endless. Rather than the endless supply of sausage rolls and party pies like some courses provide, I actually looked forward to the meal breaks!
The instructors – Andy and Amit lead a great team of instructors. Predominantly FACEMs from around Melbourne, some surgeons and pre-hospital guys also made some appearances for specific workshops and the Q&A session (which was a great chance to pick the minds of some senior guys)
The course manual – is worth the cost of the course alone I think! Provided both in PDF and iBook format (which I highly recommend) the course manual has been written by an international group of authors including Scott Weingart, Matt and Mike from the Ultrasound podcast and local FOAMed gurus like Casey Parker & Minh Le Cong as well as Andy and Amit themselves. The manual is brilliantly written, informative, easy to read and has integrated videos throughout it. E.g whilst discussing how to do a thoracotomy, clicking on the imbedded video in the manual will play a 3 minute instructive video demonstrating a cadaveric thoracotomy – without even taking you outside the manual or requiring an internet connection. The same goes for looking at CT’s of chest trauma – rather than just displaying a static image like a normal text book, clicking the picture of a sternal fracture will automatically scroll through the entire CT chest to give you a better picture of what this looks like in real life.
And now finally the big 2 questions…
Who is this course for?
I think this is the question the course is wrestling with itself. Currently there is a huge range of people attending the course, and I think this will settle down over the coming year. My answer would be though: is this course for:
A FACEM or Senior Reg who deals with trauma daily in a major trauma centre and is competent and comfortable? – probably not, but will be a valuable refresher
An intern or inexperienced PGY 2-3? – no, most of the concepts and skills were pitched well above intern level.
But how about the middle ground? How about a FACEM who works in a trauma bypass centre, who is going locuming in regional trauma centres? Or the ED Advanced trainee with minimal previous hands on/in charge experience with trauma? Or the rural GP who covers ED and manages trauma by themselves, has completed ATLS-EMST and needs an up-to-date refresher? Or the provisional ACEM 3 junior doctor just starting out in ED? Well all of this range turned up at the course in December, and all seemed to enjoy it and get something out of it.
Did I as an ED/ICU trainee who deals with trauma daily in a regional trauma centre come across anything mind shatteringly new? No, but it was still a great course in helping cement in my approach to trauma, and a great opportunity to work on communication and resus room management/leadership skills in a supportive environment. I’ve already recommended this course to my fellow registrars, and will continue to recommend it to anyone interested in improving their trauma management skills, whether they be an ED, ICU, Surgical doctor or rural GP.
Is it a replacement or competitor for EMST?
This is the hardest question… Andy and Amit say no, they aren’t trying to compete with EMST, but rather build on top of it. It’s true that pretty much the entirety of EMST is assumed knowledge in the ETM course, but briefly covered again on day one.
That said, I do think EMST has some serious competition here in Australia at least from ETM. ETM is cheaper, the waiting list is 1 month, rather than 2-3 years, it’s more up to date, and focuses on the advanced skills and thought processes needed for leading major traumas. It obviously won’t replace EMST for the surgical trainees who are required to do EMST… but for the rest of us in other specialties without mandatory requirements to do EMST/ATLS it’s an interesting question. I’d personally still recommend people do both, doing EMST around PGY2-3 and ETM a little later (or around the same time depending on where you work). But for those cash strapped and only interested in doing 1 course… I think ETM has the distinct advantage here in terms of content, delivery, cost, waiting list and of course the all important food. And EMST would never take you out and buy you a beer at the pub after a long day of thoracostomies and surgical airways 😉
I’m excited to see how ETM continues to adapt their course. One of the great benefits of being a smaller, locally run course, is that it can be tweaked and updated month by month as new evidence comes out, and as their own experience in delivering the course grows.
Dr Jeram Hyde


FINAL NOTE FROM DR TIM LEEUWENBURG
Thanks Jeram for an excellent and thorough review. I agree with the sentiments on ETM – a great course and an advancement on the usual ATLS-EMST.
This course is something new, uses early exposure to simulated scenarios (the least complex on day one would have been the ‘most complex’ on a typical ATLS-EMST) and focusses on building both practical skills and effective management of the trauma team. Equally importantly, Amit and Andy (& their colleagues) are committed to embedding relevant #FOAMed throughout he course content which will rapidly evolve.
I don’t think this is a course for newbies…as a Director for EMST I think that most of the candidates we get on a typical EMST course would have struggled on ETM. So this is a course for those who have at least some pre-existing experience in trauma or those looking for a ‘masterclass’ refresher from an enthusiastic and credible faculty (I was invited to join the instructors for dinner on day two, which was a hoot).
Will I be jumping ship from EMST to ETM? Well, Amit and Andy have offered a post as an instructor and their ethos and philosophy aligns closely with mine re: FOAMed and helping to deliver ‘quality care, out there’. So yes, I’ll be glad to instruct on ETM in future for an Australian-grown, FOAMed trauma course relevant for real world trauma.
ETM will fully meet the needs of ED CMOs, rural GP proceduralists and others who have to manage trauma teams (anaesthetic & ICU registrars etc)…but I’ll still be directing on EMST for those who need to tick it off or want an entry-level approach. And don’t worry – courses I direct tend to be a little subversive from the usual College of Surgeons mantra…
Pingback: ETM Course review by Jeram Hyde & Tim Leeuwenburg | ETM Course
Pingback: ETM course coming to Adelaide, SA - KI Doc
Pingback: ATAAC Manual - Quality FOAMed - KI Doc